
A Nurse’s Experience with the AIDS Epidemic of the 80’s
“The disease cast a long shadow over the gay community. In the first several years of what soon was called the ‘AIDS epidemic,’ a positive diagnosis was tantamount to a death sentence, and the death came at the end of months of wasting and pain.” (H.W. Brands, American Dreams, p. 254)
Interview Subject:
Wendy Waltman, age 54, former nurse who worked with AIDS patients at Beth Israel Hospital in New York from 1986-1989.
In 1985, Wendy Waltman didn’t know what exactly AIDS was, however she had heard of the disease. “The only thing I knew about AIDS before I started nursing school was Ryan White, who was a teenager in 1985 who contracted AIDS through his blood transfusions for hemophilia. “ (1) AIDS had been in New York since the early 70’s, but had evolved into an epidemic in the 80’s. The disease ripped through vulnerable communities, affecting primarily what Waltman describes as the “four h club: homosexuals, heroin abusers, Haitians and hemophiliacs.” (2) Unknown at the time, AIDS was spread through bodily fluids, and was being transmitted through unprotected sex among the homosexual community and the sharing of needles by IV drug abusers. AIDS was a death sentence for those who contracted it in the 80’s, with 19,482 deaths in New York City alone at the end of 1989. (3). Waltman worked at Beth Israel until 1989, before moving to New Hampshire. In his book, American Dreams, H.R. Brands describes 1985 through 1987 as a turning point in the AIDs epidemic, describing “the fear diminished, as science and medicine made progress against the disease”(4). Brands credits events like the National AIDS memorial quilt, the infection of Ryan White and Rock Hudson and the approval of ATZ as decreasing fears around the diseasing and ending the epidemic. However, Waltman recalls her time in Beth Israel as a time of “hysteria” (5). Her oral history challenges the national narrative of the AIDS epidemic, specifically showing how New York City felt the full force of the AIDS epidemic through the late 1980’s.
Waltman was only 19 years old when she started as a student nurse in Beth Israel hospital in 1985, and started working with AIDS patients in 1986, in the heat of the AIDS epidemic in New York. At the beginning of her nursing term, despite being 6 years into the epidemic, she nor anyone else she knew understood what exactly AIDS was and how it was spread. “When I started in 1985 we knew what AIDS was we weren’t sure what caused it, they weren’t sure how it was transmitted. The blood screening wasn’t even perfected until 1985.” (6) Beth Israel was located right in the heart of the epidemic, due to it being situated by Greenwich Village, the heart of the gay community in the 80’s and it having the second largest meth treatment facility in the world at the time. (7)
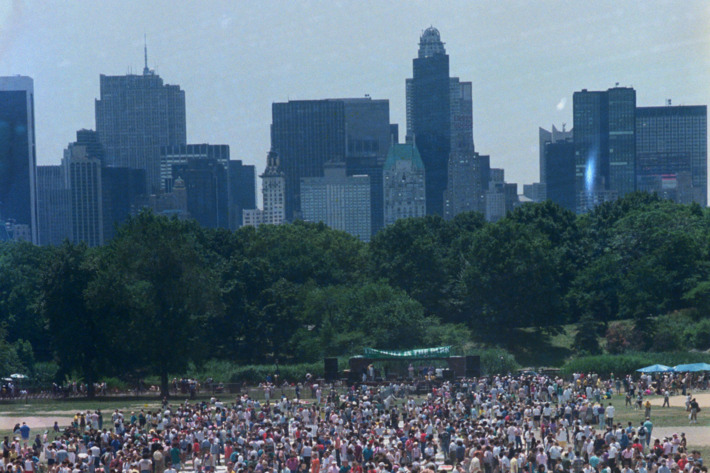
New York Memorial Quilt on Central Park’s Great Lawn, June 25th 1988. Image courtesy Bettmann/CORBIS
It’s understandable why historians such as Brands portray the AIDS epidemic ending in the late 80’s. The approval of ATZ in 1987 was a major milestone in the fight against AIDS, as it was the first drug to be clinically approved for AIDS treatment. Brands described the drug as “expensive but broadly effective.” (8). Even before with death of Rock Hudson in 1985, President Reagan had started to speak about AIDS publicly (9). Reagan’s Surgeon General released a report in 1987 that described AIDs patients as safe to interact with in an everyday capacity. (10) At the national level that Brands focuses on the condition of the AIDs community seemed to be rapidly improving from the period between 1985 and 1989.
However, the increased awareness of AIDS as a disease did not translate into better conditions or understanding for AIDS patients in New York from 1985 to 89. While on a national and federal level AIDS patients seemed to be garnering sympathy, the homosexual community that Beth Israel Hospital struggled greatly. Waltman remembers most of her AIDS patients being young, gay men. (11). “They were on their own, a lot of their families had turned their back on them and a lot of them were still afraid of losing their job in the workplace.” (12). While by 1985 the cause of AIDS had been identified, the concern that AIDS could still spread in ways that hadn’t been discovered yet was still very prevalent in common culture. (13) AIDS was described as some as the “gay disease”, and elements of the Christian right believed the gay community was, “getting what they deserved”. (14) The hysteria around the disease was not just one of health concern, but also rather the center of a cultural battle that made it difficult to bring AIDS patients into the light.
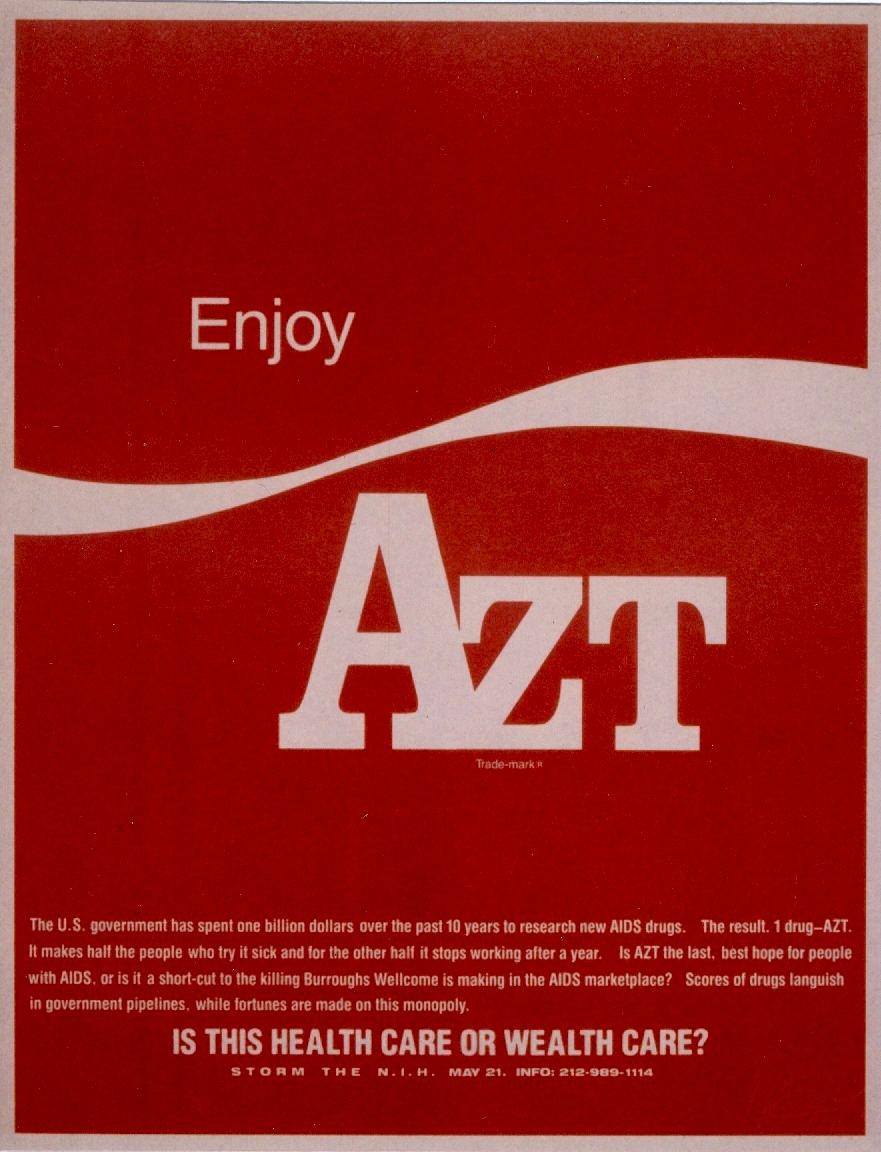
Advertisement for protest of AZT prices at the NIH- Courtesy of Liam Scheff
Further, the federal response to the AIDS epidemic proved slow. Despite AIDs research getting a major increase in funding past 1985, with Reagan declaring it a “top priority”, the actual treatment of AIDS patients during the period of 85 to 89 proved difficult. (15) These difficulties stemmed from a lack of nurses and a lack of published, uniform knowledge around AIDS. AIDS research hadn’t made its way into the nursing manuals taught to student nurses like Waltman in 1985, as the information was “too much and coming too fast” for nurses to be taught. (16) During the period of 85 to 89, there was no widely available, cheap medication for AIDS. The first cocktail widely used, AZT, cost around 8,000 to 10,000 dollars. Beth Israel patients often didn’t have the regular insurance required to afford the cocktail. (17) AIDS patients are nursing intensive patients. A HIV patient develops AIDS due to an opportunistic infection such as Kaposi sarcoma or pneumonia. This meant that nurses not only had to treat the AIDS infection, but often other nursing intensive symptoms as well. (18) On one floor in Beth Israel, a nurse was responsible for up to 18 patients, all-suffering from AIDS. (19) Beth Israel and other hospitals were unprepared for the epidemic, and faced an increasing AIDS population.
Wendy describing treating AIDS patients:
The lack of beds combined with the increasing patient load meant that there were more patients than beds. Patients were laid out the floor of rooms so that the staff of Beth Israel could attempt to treat the influx. Despite the best efforts of the nursing and medical staff, Waltman felt that, “no matter how much you were running around doing something, there was always somebody not getting what they needed.” (20) Beth Israel did attempt to improve the quality of care for AIDS patients in the hospital. An AIDS floor was developed, and a specialized AIDS intensive care unit was made in 1988. (21). However AIDS remained a terminal disease for the majority of young homosexual men who were patients at Beth Israel. Through no fault of the medical staff of the hospital, Waltman doesn’t “remember any one of my patients who I treated long term surviving.” (22)
Beth Israel is an extreme example in the AIDS narrative, as is New York in general. AIDS did not hit other areas of the US quite as hard as New York, with cities like San Francisco having better success in treating the outbreak. But by looking at New York from 85 to 89, the AIDS narrative is expanded. Despite the social and medical developments talked about by Brands, the AIDS community in New York was not experiencing a subsidence of fear, or an improvement of large scale in medical treatment. When looking at an epidemic, examining national policy and events gives the impression of uniformity of experience for those affected across the county. This process can erase the experiences of not only the professionals who worked in communities ravaged by the disease well after the end of the traditional narrative, but also those who either died or lost loved ones as a result. This oral history challenges the story that Brands and other historians tell about HIV when they present the epidemic in a national context, extending the timeline and humanizing the issues.

Aids Patient Bobbi Campbell, Courtesy of PBS
- Interview with Wendy Waltman, Lexington, KY. March 28th, 2018.
- Interview with Wendy Waltman, Lexington, KY. March 28th, 2018.
- “IV Epidemiology and Field Services Program Table 3. AIDS Diagnosis and Persons Living with HIV/AIDS by Year, Pre-1981 to 2014, New York City” (New York City HIV/AIDS Annual Surveillance Statistics 201430,2015).
- W. Brands, American Dreams: The United States Since 1945 (New York: Penguin Books, 2010), 256.
- Interview with Wendy Waltman, Lexington, KY. March 28th, 2018.
- Interview with Wendy Waltman, Lexington, KY. March 28th, 2018.
- Interview with Wendy Waltman, Lexington, KY. March 28th, 2018.
- W. Brands, American Dreams: The United States Since 1945 (New York: Penguin Books, 2010), 257.
- “Reagan, Regulation and the FDA: The US food and Drug Administrations Response to HIV/AIDS 1980-90.” (Canadian Journal Of History 44, no. 3, 2009). 467-487.
- “Surgeans General Report on Aquired Immune Deficiency Syndrome”. (US. Department of Health and Human Services, Public Health Service, Office of the Surgeon General, Rockville, MD 1986.) 5.
- Interview with Wendy Waltman, Lexington, KY. March 28th, 2018.
- Interview with Wendy Waltman, Lexington, KY. March 28th, 2018.
- Interview with Wendy Waltman, Lexington, KY. March 28th, 2018.
- Halkitis, P. N. The AIDS Generation : Stories of Survival and Resilience. (Oxford: Oxford University Press. (2014). 30.
- W. Brands, American Dreams: The United States Since 1945 (New York: Penguin Books, 2010), 256.
- Interview with Wendy Waltman, Lexington, KY. March 28th, 2018..
- Interview with Wendy Waltman, Lexington, KY. March 28th, 2018.
- Interview with Wendy Waltman, Lexington, KY. March 28th, 2018.
- Interview with Wendy Waltman, Lexington, KY. March 28th, 2018.
- Interview with Wendy Waltman, Lexington, KY. March 28th, 2018.
- “Mount Sinai Beth Israel History.” Mount Sinai Health System.
- Interview with Wendy Waltman, Lexington, KY. March 28th, 2018.
Interview:
-Phone Call, Lexington, KY, March 28th, 2018.
Selected transcript:
From phone:
Q:So you were working with AIDS patients during that period between 1985 and 1989?
A: Well yes, the thing is in 1985 when I started there there wasn’t an AIDS floor. All of the AIDS patients were mixed in on different floors. Not in the same floors but in one floor there would be, for example, a room with two AIDS patients next to a room with two elderly patients. There wasn’t a specific floor at that point for the AIDS population.
Q: Why was that?
A: In about 1981 was the first patient in Beth Israel who was diagnosed. I don’t even think they had the name AIDS yet. There was the overlying GRID, gay related immuno-deficiency syndrome. When I started in 1985 we knew what AIDS was we weren’t sure what caused it, they weren’t sure how it was transmitted. The blood screening wasn’t even perfected until 1985. It was sort of that the patients presented themselves. It was a 900 bed hospital, of course they would have to go to a medical ward. There was no ward to keep it separate.
Q: So you didn’t know how it was transmitted (when you started working at Beth Israel) in 85?
A: No one knew how it was transmitted. They weren’t sure how it was transmitted. It was still at the point were they didn’t know if kissing transmitted it, if it was transmitted through salvia. No one knew how this was transmitted, none of the infectious disease doctors knew either
Q: Can you describe some of the difficulties with working with AIDS patients during the period you worked with them?
A: When I started in the fall of 1985, maybe 15 to 20 percent of a regular floor would be AIDS. By the time I graduated the two year medical program it was around 40-50. So it was a massive change in a little amount of time. This was before any of the vaccinations. Realize that this was also in the middle of a nursing health crisis and these patients were incredibly complex to have on the floor. None of the staffing was changed to help out in that way. It was a really hard time to be a nurse on any floor. In 1986 when a young man came in there would be several things they would present with. Just because you were HIV positive didn’t mean you had the disease, you had to have something in addition to it, an opportunistic infection. None of this in 1985 was written in books. This was not in the normal one thousand page nursing tome that you had. It was all so fresh and coming so fast. The patients who came in were HIV positive and had an opportunistic infection. These were nursing intensive patients. One of the infections that many patients had was kaposi sarcoma which was a rare skin cancer. The other thing they would have was bloody diarrhea, diarrhea which is actually unimaginable to the normal person. You’d have a patient with both of these things going on the same time. If you were a registered nurse you had a third of the floor to deal with on top of this. If you were on evening or night shift you had half of the floor. This was before the specialized AIDS unit opened up. You’d have anywhere between 16 to 18 patients. On top of these complicated AIDS patients you’d have your normal patients who you also need to take care of. There just wasn’t enough help. I personally felt that I wasn’t doing enough, no matter how much you were running around doing something, there was always somebody not getting what they needed.
Q: So the patients weren’t getting the treatment they needed?
A: Nobody was getting the treatment they needed. There wasn’t an effective nursing to staff ratio. Everyone was trying and nobody was getting enough. You had interns who were just out of medical school pulling 24-36 hour shifts. Sometime as a nurse in New York City you would call a intern for help and they had already been up 24 hours. It was difficult to put it mildly.
Timeline:
Leave a Reply