Mike Aimino & Lisa Freeman
Summary of:
Clement, L.C., Avila-Casado, C., Macé, C., Soria, E., Bakker, W.W., Kersten, S. & Chugh, S.S. (2011). Podocyte-secreted angiopoietin-like-4 mediates proteinuria in glucocorticoid-sensitive nephrotic syndrome. Nature Medicine, 17(1), 117-122. doi: 10.1038/nm.2261.
What is Nephrotic Syndrome?
Nephrotic syndrome is a condition that causes proteinuria, hypoalbuminemia, edema, hyperlipidemia, and lipiduria in individuals that have it. Proetinuria and lipiduria are when there are proteins and lipids in the urine, respectively. Hypoalbuminemia is when there is a low amount of albumin in the blood while hyperlipidemia is when there are high amounts of lipids in the blood. It can be caused by diabetic nephropathy, minimal change disease (MCD), focal and segmental glomerulosclerosis (FSGS), or membranous nephropathy. MCD is the primary cause of nephrotic syndrome in pre-adolescents, making up 85-95% of the cases. About 15 in 100,000 children have MCD with 2-7 new cases annually in 100,000 children. The prevalence of MCD is much lower in adults, making up only 10-15% of the cases. MCD is sensitive to glucocorticoid treatment, while the other diseases show a varied response, making it a good target to study.
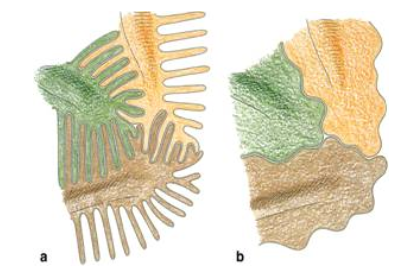
Other complications of nephrotic syndrome include foot process effacement of podocytes. Normally, podocytes extend primary processes to the glomerular basement membrane (GBM) of the capillaries. Foot processes extend from the primary processes and lie on the GBM. Adjacent foot processes then interdigitate, which looks similar to locking your fingers together (pictured below). In individuals with necrotic syndrome, the foot processes disappear, making it look like the cell membrane is continuous. This leaves spaces between podocytes which allows proteins to leave and enter the urine.
All angioproietin-like proteins (Angptl) are glycoproteins that are sensitive to glucocorticoids. Angiopoietin-like proteins have been found to play a role in the development of hypertriglyceridemia and tumor metastasis. They have many different effects on cells depending on the part of the body in which they are found. Angptl4 is an inhibitor of lipoprotein lipase and has an effect on triglyceride levels in the blood. There has been no previous research to show that Angptl4 plays a role in proteinuria.
Question
What role, if any, does Angptl4 play in proteinuria associated with nephrotic syndrome?
Approach
The researchers employed a large arsenal of experiments and analysis techniques, so we will only give an overview of the experimental approach here. They started by evaluating four different nephropathy models, each model simulating a different disease that causes nephrotic syndrome. They identified the model that yielded the greatest increase in Angptl4 expression (puromycin nephrosis, or PAN), and used this model in later experimentation. They then studied a previously established Angptl4 transgenic mouse model and developed two new transgenic rat models. The NPHS2-Angptl4 model is characterized by upregulated Angptl4 in podocytes, while the aP2-Angptl4 is characterized by an upregulation of circulating Angptl4, secreted from adipose tissue. They evaluated Angptl4 expression and morphological changes for each model.
Although data for the aP2-Angptl4 is presented in supplemental materials, the remainder of the paper is focused on continuing experimentation with the NPHS2-Angptl4 model. With this model, they measured albuminuria in rats at varying ages. They then induced PAN, a model for minimal change disease (MCD), and measured albuminuria again. To analyze an additional variable affecting protein expression, they treated the rats with glucocorticoids after inducing PAN and measured resulting proteinuria and Angptl4 expression. Finally, the researchers conducted an in vitro study in two different cell lines of the sialylation of Angptl4 on its electrophoretic migration and the level of proteinuria occurring in the transgenic models.
A variety of analysis techniques were utilized throughout the experiments described above. Light microscopy and electron microscopy were used to analyze morphological changes at the glomerular and cellular levels, respectively. Immunohistochemistry with confocal microscopy and immunogold electron microscopy were used to localize and quantify Angptl4 expression. The researchers used SDS-PAGE to detect urinary protein and a combination of 2-D gel electrophoresis and western blotting to differentiate between forms of Angptl4.
Main Findings
A key result from these experiments was that increased expression of podocyte-secreted Angptl4 (NPHS2-Angptl4 transgenic model) caused increased proteinuria, similarly to proteinuria observed in rat models and human MCD patients. Angptl4 expression was also associated with morphological changes characteristic of MCD. More specifically, proteinuria was induced when the glomerular basement membrane (GBM) showed the presence of Angptl4, even though the podocytes did not yet show morphological changes. The researchers interpreted these results as an indication that Angptl4 causes a defect in the GBM that ultimately leads to proteinuria. They also found that Angptl4 decreased after glucocorticoid treatment. Finally, their results showed that sialylation of Angptl4 was associated with decreased proteinuria.
Broader Context
The results show that in the PAN model there is a 60-80 fold upregulation of glomerular Angptl4 expression in the PAN model. This is close to the 120 fold increase found in the NPHS2-Angptl4 heterozygous, male rats, meaning that it is a good model for studying nephrotic syndrome. This model is the first demonstration of the important role Angptl4 plays in proteinuria. Because the NPHS2-Angptl4 rats had reduced albuminuria when fed with ManNac and had an increase in the sialylation of glomerular Angptl4, it suggests that hyposialylation could be a mechanism by which Anglt4 overexpression causes proteinuria. Therefore, treatment with sialic acid precursors could be a potential therapy for individuals with some forms of nephrotic syndrome, particularly minimal change disease.
References
2. National Institute of Diabetes and Digestive and Kidney Diseases. Glomerular Disease Primer: The Normal Kidney. http://www.niddk.nih.gov/research-funding/at-niddk/labs-branches/kidney-disease-branch/kidney-diseases-section/glomerular-disease-primer/-normal-kidney/Pages/normal-kidneys.aspx
I find this article very interesting, especially as I had not learned about podocyte function previously. I would like to learn more about how the secretion of high-pI Angpt14 can facilitate its tethering to the GBM and its role in binding heparan sulfate proteoglycans.
I was totally with this article until they started talking about sialylation and the charge on the protein. I wasn’t really sure how to interpret the data shown in figure four, although I understand a 2D gel electrophoresis in concept. I couldn’t tell what each band was. It is interesting that the authors started their research pretty broadly, first testing Angptl4 mRNA levels across several disease causing conditions. This makes me think that this research was very novel, and that there is room to explore the topic beyond the scope of this paper.
I found this article to be very informative in a lot of ways. I do think that the format was a little strange and made the paper more difficult to follow because of the lack of subheadings. There were a few things that stuck out to me in the paper as I read. One of which was that in Figure 3, they briefly mentioned that heterozygous females were not albuminuric. I wonder if this was something they expected or was a new finding. I did find Figure 4 more confusing than the rest and am looking forward to your breakdown of the figure. I also found the idea of hyposialylation as a factor that causes overexpression of Angptl4 leading to proteinuria to be an interesting idea, and I do think they have the beginnings of supporting evidence for this. The last thing I wanted to mention that I did not care for with the paper was the large amount of supplemental figures that were referenced. They seemed to have a great deal of valuable evidence through which they gathered a lot of conclusions and it may have been more beneficial for that to be present within the paper rather than as supplements in some cases.
I thought this paper was engaging. I felt all of the different models, causes of disease, and experiments they used were great. I was intrigued by the order in which their experiments were conducted. They first used mouse models and ended with in vitro work–why would they conduct experiments in mouse models before using cell-lines? Additionally, I was a bit confused by figure 4. I could not concur with their interpretations of the results.
I am interested in the sialylation and Angptl4 mechanism. Moreover, how the increase or decrease in sialylation can cause Angptl4 overexpression which contributes to proteinuria. I am curious how increased amounts of sialic acid precursors decrease podocyte-secreted Angptl4 that is a contributor in proteinuria in variations of nephrotic syndrome.
This article is very interesting and definitely introduces some new concepts that I have not studied previously! I am also a little bit confused by the concept of sialylation. I don’t really understand how sailic acid precursors could be therapeutic targets. On a different note, I really did not like the organization of this article. I found it pretty difficult to navigate without subsections or structure.
Why would this disease be more prevalent in children than adults? Would this disease be related to issues of kidney development in childhood and adolescence? Additionally, I think that the information given in this paper is kind of scattered which makes it hard to read but overall, the results were clearly explained so I understand what was learned from this study. However, the experimental approach could have been better explained in regards to the various mouse models.
I think the findings of this paper are definitely really interesting, but the way this paper was designed/written really makes it hard to comprehend. I have been warned by previous professors that Nature papers are incredibly dense, though. Like others, I was a bit confused by this idea of sialylation and therefore am not entire sure how treatment with sialic acid precursors could be therapeutic. I look forward to hearing how this is explained!
The feature of podocyte function was really interesting and I enjoyed being able to apply my (very limited) previous knowledge from Bio 120 regarding their role in renal physiology. The authors touch on a number of different models and look at things pretty broadly which lends themselves to further and deeper explanation on this topic. Though the breadth of their paper was interesting to see, some of their data was confusing, specifically for me – Figure 4. Toward the end the authors point out different facets of Angpt14 expression, and I’d love to know more about how this information can be applied to different facets for AD as well as other organs and functions.
It appears as if over-expression of Angptl4 leads to hyposialyation therefore preventing it from interacting with the GBM appropriately leading to problems with podocyte interaction and protein leakage into the urine. I can imagine that the glycosylation process is being overwhelmed by the overproduction of this protein, but why can’t the fraction that gets properly sialyated function in the GBM? Figure 4b shows an increase in both sialyated and non-sialyated protein in the PAN model of disease.
I like the fact that they investigated Angptl4 gene in vitro and in vivo with ManNAc. I also like the fact that not only they looked at Angptl4, they also looked at NPHS2. However, I was confused how to interpret figure 4. Other than doing western blot with blurry images, I think they could have done other methods to test the hypothesis. I also think the method section could be divided more (where they could have separate western blot section). The result and discussion were combined together from this Nature Medicine article. I think this was little bit different type of paper unlike we had in past. Also, not only test transgenic mice in PAN, maybe they could have test the similar effect in different cell types. They could have drawn the model systems in order to help readers to understand what they are talking about. They talked about the glomerular expression of Angptl 4 was glucocorticoid sensitive and was highly unregulated in the serum from the models of MCD.
I found the connections shown in figure 3 to be of particular interest. The ability to create a precise transgenic model for this disease was key for the research and findings seen in this study, like the selectivity of proteins in the filtrate of the urine in transgenic animals. I would be interested to learn more (and understand) the background information regarding figure 4. it seems like there is a large volume of data present, but is a bit difficult to interpret.
In this experiment they make the general claim that the effectiveness of the two models are interchangeable as the PAN model shows a 60 to 80 fold increase in the up-regulation of glomerular Angptl-4 in comparison to the 120 fold increase seen in NPHS2-Angptl-4, heterozygous, male rats; what is it that makes a 60-80 fold increase close enough to be considered a “good model”? Also I am curious to at this stage in the research how implementable are these treatment and therapy ideas? I would also be interested in investigating more about the specific mechanism in which sialic acid inhibits the proteinuria… Overall I found this article very interesting and unique because of the specific content that it is covering.
The article is truly inspiring, thank you for sharing! Free Related 1Z0-819 Certifications questions are shared. Good luck with your exam preparation!
Truly a remarkable read, thank you for sharing this brilliant article. The Valid real D-PST-OE-23 exam test was the key to unlocking my promotion and raise. Grab it for free today!
Itcertkr는 유일하게 여러분이 원하는Microsoft인증DP-100시험관련자료를 해결해드릴 수 잇는 사이트입니다. Itcertkr에서 제공하는 자료로 응시는 문제없습니다, 여러분은 고득점으로 시험을 통과할 것입니다.
選擇最適合的ServiceNow CIS-CSM題庫學習資料,并來獲得認證,它能加速您在信息技術行業里快速成長,也是加薪升遷的成功選擇。在取得您第一個CIS-CSM認證后,您還可以參加其它的IT認證考試,PDFExamDumps的考古題能幫助獲得更多的成功。我們擁有超多十年的IT認證經驗,在我們的支援下,您可以順利的ServiceNow CIS-CSM考試。我們還承諾,對于使用我們CIS-CSM考古題失敗的考生,將提供100%無條件退款。
The content of the article is thought-provoking, and I’ve learned a lot from it. Here are the New test camp C_SAC_2402 materials materials, free of charge—best of luck!
The article was truly wonderful; thank you for sharing it! Free Top C_C4H46_2408 exam dumps resources for exam success. Wishing you the best!
I really appreciate your article, it was so enlightening and refreshing. Exam 2V0-32.22 study solutions has outstanding content, and I hope it helps you, at no cost.
The article was a breath of fresh air in terms of insight. This HPE0-V22 latest test dumps.zip helped me get promoted and earn a pay raise. Now it’s free for everyone. Best wishes for your career advancements!
私たちの250-580練習問題は実際に自分の魅力を持っているため、世界中のユーザーを引き付けました。250-580練習問題のように、あらゆる面でユーザーのニーズを真剣に検討する練習問題がないです。250-580練習問題を利用すれば、250-580試験に合格することは夢ではないです。従って、ためらわなくて、250-580練習問題を購入し、勉強し始めましょう!
It was one of the most beneficial pieces I’ve read in a while. I advanced with the help of the Reliable exam C_THR88_2405 pass4sure, and now it’s free for everyone. Best wishes for your career promotions!
Your article has really expanded my perspective, thank you. Ready to tackle the Test DP-300 questions vce exam. Wishing for good results!
In der heutigen wettbewerbsorientierten IT-Branche hat man viele Vorteile, wenn man die SAP C-THR85-2411 Zertifizierungsprüfung besteht. Mit einem SAP C-THR85-2411 Zertifikat kann man ein hohes Gehalt erhalten. Menschen, die SAP C-THR85-2411 Zertifikat erhalten, haben oft viel höheres Gehalt als Kollegen ohne SAP C-THR85-2411 Zertifikat Jedoch ist es nicht sehr einfach, die SAP C-THR85-2411 Zertifizierungsprüfung zu bestehen. So hilft ZertFragen Ihnen, Ihr Gehalt zu erhöhen.
This article is truly magnificent, thank you for sharing your knowledge. Explore C-C4HCX-2405 certification dump with its rich content, available free for your benefit.
What a thought-provoking and inspiring read, thank you for sharing! 030-100 latest exam questions answers offers great insights, and it’s completely free to access.
What a brilliant article, I’m so grateful for your generosity. Boost your IT skills and enjoy free Latest test aPHRi discount voucher. Best of luck to you!
Wollen Sie Ihre Fähigkeit beim Lernen der Microsoft AZ-500 Zertifzierungsunterlagen verbessern und sich von anderen besser anerkannt? Microsoft Prüfungen helfen Ihnen, Ihre Fähigkeit zu verbessern. Wenn Sie die AZ-500 Zertifizierung besitzen, können Sie Ihre Arbeit besser erledigen. Obwohl die AZ-500 Prüfung sehr schwierig ist, können Sie sich nicht um die Vorbereitung der Prüfung sorgen. Nach der Nutzung der DeutschPrüfung AZ-500 Dumps können Sie die Microsoft AZ-500 Prüfung zu bestehen und auch die entsprechenden Kenntnisse beherrschen.
Unser ZertSoft stellt Ihnen die besten Fragen und Antworten zur Network Appliance NS0-516 Zertifizierungsprüfung zur Verfügung und führt Ihnen schrittweise zum Erfolg. Die Schulungsunterlagen zur Network Appliance NS0-516 Zertifizierungsprüfung von ZertSoft werden Ihnen eine reale Prüfungsvorbereitung bieten. Sie sind ganz zielgerichtet. Sie werden sicher ein IT-Expert werden. Unsere Network Appliance NS0-516 Schulungsunterlagen sind Ihnen am geeignetesten.Tragen Sie doch in unserer Website ein. Sie werden sicher etwas Unerwartetes bekommen.
Thank you for sharing such an inspiring and impactful article! The Reliable MLS-C01 test book materials are first-rate, and they’re available for free.
そうでなければ、時代遅れになるリスクを負います。当社のMB-230認定テストは、技術スキルを向上させ、さらに重要なこととして、厳しい労働環境で明るい未来のために戦う自信を高めるのに役立ちます。当社の専門家は、MB-230学習ツールの開発に多くの時間とエネルギーを費やしています。あなたは私たちを信頼し、あなたの将来の発展において私たちをあなたの正直な協力者にすることができます。参考までに、MB-230試験の利点をいくつかご紹介します。
I love how inspiring this article is, thanks for sharing! Wish me the best of luck for my C-TFG61-2405 vce torrent exam!
tornado 15k
Your article was very memorable, thank you for sharing it. Sharing the Reliable C_S4PPM_2021 visual cert test test that was a key factor in my promotion and salary increase. It’s free for you today—hope you achieve your professional dreams!
I walked away from that article with a deeper understanding. Explore the valuable content in CTFL-Foundation download free dumps, provided for free to assist you.
当社GoShikenは、製品の品質が非常に重要であることを深く知っているため、AZ-305テストトレントの高品質の開発に注力しています。当社の製品を購入したすべてのお客様は、AZ-305ガイド急流に深い印象を残しています。もちろん、顧客は製品の高品質だけでなく、製品の効率性にも深い印象を残しています。 AZ-305試験の質問は多くの時間を節約するのに役立ちます。AZ-305試験準備を使用する場合、学習に20〜30時間を費やすだけで、AZ-305試験に合格できます。
Thank you for the brilliant share, it really left me in awe! The 020-100 demo test resource is packed with content and made available for free to help you.
No hesitation, this is deserving of a like. Best wishes for your exams! Here’s the free 200-301 latest exam collection sheet material.
Einige Websites bieten auch die neuesten Lernmaterialien zur The Open Group OGBA-101 Prüfung im Internet. Aber sie haben keine zuverlässigen Garatie. Ich würde hier sagen, dass It-Pruefung einen Grundwert hat. Alle The Open Group-Prüfungen sind sehr wichtig. Im Zeitalter der rasanten entwickelten Informationstechnologie ist It-Pruefung nur eine von den vielen. Warum wählen die meisten Menschen It-Pruefung? Dies liegt darin, die von It-Pruefung gebotenen Prüfungsfragen und Antworten wird Sie sicherlich in die Lage bringen, das Exam zu bestehen. wieso? Weil es die neuerlich aktualisierten Materialien bietet. Diese haben die Mehrheit der Kandidaten schon bewiesen.
The content is excellent, so I’m liking it now. I used the 156-536 reliable soft simulations to secure a promotion and raise. Now, I’m offering it for free. Wishing you all success in your careers!
This article is very insightful and has given me a lot of inspiration. Improve your IT skills and access free HPE0-V26 valid exam study guide. Wishing you the best of luck!
Die Schwierigkeiten können den Charakter eines Menschen testen. Eine schlechte Situation kann die Aufrichtigkeit eines Menschen zeigen. Wenn man einer schlechten Situation gegenüberstehen, können nur die mutigen es gant leichtnehmen. Sind Sie ein mutiger Mensch? Wenn Sie sich nicht so gut auf Ihre Prüfung vorbereiten, können Sie es noch leichtnehmen. Weil Sie die Fragenkataloge zur SAP C-C4H62-2408 Prüfung von DeutschPrüfung haben. Und eine SAP C-C4H62-2408 Prüfung wird Sie nicht niederschlagen.
This is a truly extraordinary piece of work, thank you for sharing. With Reliable C-THR88-2405 exam preparation, you get comprehensive material available for free to support you.
Such a brilliant article, thank you for sharing this gem with us. Strengthen your IT skills with free Online Google-Workspace-Administrator bootcamps. Wishing you the best of luck!
商品を購入するとき、信頼できる会社を選ぶことができます。我々ShikenPASSはH3CのGB0-392試験の最高の通過率を保証してH3CのGB0-392ソフトの無料のデモと一年間の無料更新を承諾します。あなたに安心させるために、我々はあなたがH3CのGB0-392試験に失敗したら全額で返金するのを保証します。ShikenPASSはあなたのH3CのGB0-392試験を準備する間あなたの最もよい友達です。
Great content, without a doubt, I’m clicking that like button. Sharing Latest exam camp H13-511_V5.5 file materials for free—boost your career with these essential resources!
The article is very empowering, thanks for sharing! The Reliable CMRP test guide materials questions are crucial for your promotion and salary raise—now available for free!
ANC-301試験問題により、3つのバージョン、PDFバージョン、PCバージョン、APPオンラインバージョンが強化されます。学習するANC-301学習ガイドの最適なバージョンを選択できます。 ANC-301トレーニング準備の各バージョンは、さまざまな特性とさまざまな使用方法を後押しします。たとえば、ANC-301ガイドトレントのAPPオンラインバージョンは、Webブラウザに基づいて使用および設計されており、ブラウザを備えたあらゆる機器で使用できます。試験シミュレーション、時間制限試験、および間違いの修正の機能を強化します。
I love the way you write and share your niche! Very interesting and different! Keep it coming!.
Actually I read it yesterday but I had some thoughts about it and today I wanted to read it again because it is very well written. I have really enjoyed reading your blog posts.
I’m truly thankful for your article, it left a lasting and meaningful impression. Good luck on your exam! Here are the free L4M5 latest exam topics resources.
Your article is simply remarkable, thank you for sharing it! The Discount 1Z0-921 code content is amazing, and you can get it for free.
誰もが私たちの人生の貴重を認識する必要があります。時間を無駄にすることはできないので、目標をまっすぐに達成するための良い方法が必要です。もちろん、最新のGMOB試験トレントが最適です。 GMOB試験の質問から、認定試験の知識だけでなく、質問に迅速かつ正確に回答する方法を学ぶことができることをお約束します。今、GMOBテストトレントのデモを無料でダウンロードして、すばらしい品質を確認できます。
The content is impressive, definitely worthy of a like. Certification 1z0-1162-1 dumps offers premium content, and it’s available to you at no charge.
This article has given me many new ways of thinking, and it’s really useful. Sharing the CTAL-TM-001 valid exam pass4sure questions for free, the key to your career growth!
I’m all about this content—definitely liking it. Sharpen your IT abilities with free 1z0-1073-24 latest mock exam. Wishing you the best of luck!
Your article was really impressive, thank you for this insight. With PMP valuable feedback, you get comprehensive material available for free to support you.
This article is brilliant, and I’ve gained many insights from it. Good luck to me on my MLA-C01 free sample questions exam! Hoping for great results!
Your article was a true standout, I’m really grateful for it. The Valid examcollection N10-009 test helped me secure my promotion and raise—grab it for free today!
Your article is truly amazing, I appreciate you sharing it. Using this Study C_C4HCX_2405 Notes, I earned a promotion and raise. Now, it’s free for everyone. Best of luck in your career growth!
I can’t thank you enough for your article, it really resonated with me. Here’s the free Reliable test AD0-E502 collection pdf test content. Wishing you success!
I’m so thankful for your article, it was a real game-changer. N10-009 dumps cost helped me achieve a promotion and salary boost. Get it for free today!
I truly appreciate your article, it is stunning! The Trustworthy D-PVM-OE-01 dumps exam is almost here. Please send me good vibes!
This article gave me a new perspective, thank you for sharing! The Reliable test Community-Cloud-Consultant test content is excellent, and you can access it for free.
Your article was remarkable, I’m truly thankful for it. Free access to CV0-003 valid practice questions, full of rich content, is available to enhance your studies.
This kind of clever work and reporting! Keep up the terrific works guys I’ve included you guys. download s25 ultra user guide
The article was incredibly valuable to me. Get free H19-423_V1.0-ENU latest real test questions to improve your IT knowledge. Wishing you success!
I deeply appreciate your article, it’s left a lasting mark on me. Free New test MLS-C01 camp pdf questions—your key to promotions and higher earnings!
By reading this article, I have gained a deeper understanding of this field. The 500-710 valid test pattern test questions are free! Wishing you all the best of luck in your exams!
Der Kundendienst ist ein wichtiger Standard für eine Firma und Zertpruefung bemüht sich sehr dafür. Nachdem die Kunden GRI ESRS-Professional Prüfungsunterlagen gekauft haben, geben wir ihnen rechtzeitiger Bescheid über die Aktualisierungsinformation der GRI ESRS-Professional und schicken die neueste Version per E-Mail. Dieser Aktualisierungsdienst ist innerhalb einem Jahr gratis. Wir sind getrost mit unseren Produkten. Deshalb garantieren wir, falls Sie nach dem Benutzen der GRI ESRS-Professional Prüfungsunterlagen die Prüfung nicht betehen, werden wir Ihnen mit voller Rückerstattung unser Bedauern zeigen.
MogiExamが提供しておりますのは専門家チームの研究したCCAK問題と真題で弊社の高い名誉はたぶり信頼をうけられます。安心で弊社の商品を使うために無料なCCAKサンブルをダウンロードしてください。
Thank you for sharing; it was truly incredible! Exam IDFX quizzes provides free, abundant content, designed to help you succeed.
今働いている受験者たちは悩んでいるのでしょう。時間と精力の不足を感じますか?SCP-NPM試験は重要な試験だから、十分の時間と精力を利用して試験を準備します。弊社の問題集は質高いので、お客様はJapancertのSCP-NPM問題集を利用したら、少ない時間と精力で試験に気楽に合格することができます。躊躇わずに我々のSCP-NPM問題集を購入してください。
I gained immense value from that article. The Latest braindumps GB0-382 ebook questions were key in securing my promotion and raise—now it’s your turn! Get them for free!
I’m deeply grateful to NaturePath Herbal Clinic for the remarkable improvement in my Amyotrophic Lateral Sclerosis (ALS) condition. Prior to starting their ALS Herbal Treatment program, my health was declining rapidly. After few months on their ALS Herbal treatment program, I’ve seen major progress, I can now walk independently, and my speech has significantly improved. Visit http://www.naturepathherbalclinic.com.
What an insightful article, I truly appreciate your sharing it! About to take the 1z0-1033-24 valid exam questions and answers exam! Let’s hope everything goes smoothly!
This article is outstanding, I’m so grateful for your sharing. Ethics-In-Technology valid free study questions offers valuable insights, and it’s all free.
It was a truly rewarding and enlightening piece of writing. The New Databricks-Certified-Professional-Data-Engineer test pdf was the key to my promotion and raise. Now it’s free to everyone. Wishing you all a successful career boost!
This article has made me reflect on many things, and I’ve learned quite a bit. Get free New CPP-Remote braindumps to enhance your IT expertise. Wishing you success!
It opened my mind in ways I didn’t expect. Free Exam CEM sample test papers for everyone—good luck!
I’m truly grateful for your article, it left an indelible mark. Wishing you all the best! Here’s the free H12-831_V1.0 reliable dumps book material.
This is a truly magnificent article, thank you for sharing your thoughts. The Customized CPQ-301 Lab Simulation test questions are free, and they’re the key to your next promotion!
What an outstanding article, thank you for this insightful share. The XSIAM-Analyst new dumps sheet helped me secure a promotion and salary raise. Now it’s free to all. Best wishes for your career advancements!
So good, I’m liking it without any delay. We are offering Latest Google-Ads-Video exam camp, full of valuable content, for free, hoping it proves helpful.
あなたはHealth-Cloud-Accredited-Professional試験を準備していて精確の資料がありませんなら、我々ShikenPASSの資料を参考しましょう。我々はあなたが一発で試験に合格するのを保証します。我々は試験に対応する弊社のHealth-Cloud-Accredited-Professional問題集を継続してアップグレードしています。あなたの持っているすべての商品は一年の無料更新を得られています。あなたは十分の時間でHealth-Cloud-Accredited-Professional試験を準備することができます。
I’ve been living with Parkinson’s disease for quite some time, and for years, I struggled to find lasting relief. While medications offered some temporary help, the symptoms always returned and often worsened.Out of a mix of hope and hesitation, I decided to try an herbal treatment program from NaturePath Herbal Clinic. I’ll admit, I was skeptical at first. But around the fourth month, I began to notice real, steady progress.my tremors became less frequent the stiffness in my body eased My balance and coordination gradually improved It wasn’t an overnight transformation, but it was consistent and life changing. For the first time in years, I feel more in control of my body. I can move with greater freedom, sleep more peacefully, and enjoy daily activities without the constant discomfort I once accepted as normal.The improvement I’ve experienced physically, emotionally, and mentally has been nothing short of upliftings.If you’re exploring natural options for managing Parkinson’s, I wholeheartedly recommend looking into NaturePath Herbal Clinic. Their approach has made a real difference in my life, and I’m truly grateful I gave it a chance. www. naturepathherbalclinic .com
I’m amazed by the depth of your article, thank you for sharing! The NetSec-Generalist new test collection file helped me secure a promotion and raise. Now, I’m giving it away for free. May your career paths be filled with success!
Your article was really impressive, thank you for this insight. The 350-401 latest practice test online helped me with a promotion and raise. Now it’s free to everyone. May your career progression be swift!
That article was a real eye-opener for me. I’m taking the Regualer ITIL-4-Practitioner-Release-Management update exam soon. Fingers crossed for success!
我們Fast2test Peoplecert的DevOps-Foundation的考試考古題是經過實踐檢驗的,我們可以提供基於廣泛的研究和現實世界的經驗,我們Fast2test擁有超過計畫0年的IT認證經驗,DevOps-Foundation考試培訓,包括問題和答案。在互聯網上,你可以找到各種培訓工具,準備自己的DevOps-Foundation考試認證,Fast2test的DevOps-Foundation考試試題及答案是最好的培訓資料,我們提供了最全面的驗證問題及答案,讓你得到一年的免費更新期。
I’m truly amazed by the depth of your article, thank you for sharing! Here are the New CSP-Assessor test questions pdf questions for free—your key to career advancement!
Betflix Slot Auto Wallet PG Betflik ทางเข้า สล็อต ฟรี 50 รับ 100
Slot Wallet Auto Slot True Wallet ฝาก – ถอน ไม่มีขั้นต่ํา 2025
Betflix slot wallet iwallet link login ทาง เข้า สู่ ระบบ
Slot Wallet iWallet Link Login เข้าสู่ระบบ สล็อตวอเลท
I was diagnosed with ALS four years ago. For over two years, I relied on prescription medications and therapies, but unfortunately, the symptoms continued to worsen. My mobility declined, muscle weakness increased, and I experienced growing fatigue and discomfort that affected my daily life.
Last year, out of desperation and hope, I decided to try an herbal treatment program from NaturePath Herbal Clinic. Honestly, I was skeptical at first, but within a few months of starting the treatment, I began to notice real changes. My energy improved, the discomfort eased, and I felt stronger and more capable in my daily life.Incredibly, I also regained much of my stamina, balance, and confidence. It has truly been a life-changing experience I feel more like myself again, better than I’ve felt in years. If you or a loved one is struggling with ALS, I sincerely recommend looking into their natural approach. You can visit their website at www. naturepathherbalclinic .com
I’m deeply thankful for your article, it left a lasting effect. I’m soon to face the Latest test 220-1202 tutorial exam. Hope I do well!
Thank you for sharing this article, it’s incredibly motivating! The HQT-6714 valid braindumps book questions are free—unlock your promotion and salary raise!
What a fantastic and inspiring article, thanks for sharing! Valid New-Jersey-Real-Estate-Salesperson test camp helped me land a promotion and salary increase. Now, I’m giving it to you for free!
After reading this article, I’ve gained a new perspective on how to look at the problem. The Valid study SC-400 questions sheet questions were essential to my promotion and salary boost, and today, I’m sharing them with you for free!
I’m truly grateful for your article, it really made a mark on me. Latest DP-300 test syllabus helped me get promoted and get a pay raise. Now, I’m sharing it with you for free today!
Thank you for sharing this eye-opening article! The PMP exam consultant questions were a key part of my success—promotion and salary raise—and today, I’m sharing them for free!
The article was a breath of fresh air in terms of insight. Almost time to face the Exam CISM preview exam. Wish me good luck!
手上能拿到一些實用的認證證書,無疑為自己的就業開拓了一番新的領土和創造了一些機會。CDCP 是全球最大的網絡設備公司 EXIN 公司的認可的初級技術認證,在整個 EXIN 認證體系中處于售前規劃方向的基礎證書,有了CDCP 認證你的平均年薪將不低于10萬人民幣。雖然獲取 CDCP 認證需要投入額外的時間與金錢,但事實證明IT認證的投入產出是值得的,對於未來的職業發展非常有利。
Thank you for sharing this article, it’s incredibly motivating! You’ll find the ISO-IEC-27001-Lead-Implementer latest test answers content valuable, and it’s completely free to access.
I’m truly grateful for your article, it really made an impression. Strengthen your IT abilities with free AZ-900 test questions vce. Good luck with your exams!
The content is just that good—instant like from me. Enhance your IT knowledge with free New Analytics-Con-301 test registration. Best of luck on your exams!
Such an incredible article, I’m thankful for your generosity in sharing it. “Razz Bar 10000 Puffs” vienkartiniai garintuvai – pakartotinai užpildomi aliejumi su tinklelio spirale – didmeninė ir didmeninė prekyba vienkartiniais garintuvais
This article is so encouraging, thanks for sharing it! The Latest C_THR92_2505 test online helped me move forward in my career with a promotion and salary increase. Now, I’m sharing it for free. Wishing you career success!
Your article is truly stunning, thank you for sharing! Free AgilePM-Foundation certification exam dumps study materials—best of luck with your studies!
I’m in total awe of your article, thank you for letting us read it! Unlock the door to promotions and salary raises with the free Latest C-S4PM-2504 test answers questions!
This article is absolutely enlightening, thank you for sharing! Thanks to the 1Z0-1085-25 test score report, I received a promotion and salary increase. It’s free now for everyone. Wishing you all success in your careers!
It was such a valuable learning experience. The Study 71201T group resources are available for free—good luck, everyone!
Truly an impressive article, I’m grateful for your share. Sharing the QSA_New_V4 knowledge points test that led to my promotion and raise, now free to all. Best wishes in your pursuit of career success!
Thank you for your article, it was so insightful and inspiring. About to take the Reliable NSE7_OTS-7.2 exam collection free exam! Let’s hope everything goes smoothly!
I’m absolutely loving this content, giving it a like. This is the Media-Cloud-Consultant exam simulator online exam I passed for my promotion and salary raise. It’s free for you today—hope you reach your career milestones!
Your article is absolutely mind-blowing, thank you for sharing it! Razz Bar 30000 Puff Vape za ponovno polnjenje | 16 okusov | 650mAh USB-C – Veleprodaja in množični nakup za vapes za enkratno uporabo
Your article took my breath away, thank you for sharing! Elfbox 14000 Puffs Recargable Vape desechable con bobina de malla y 25mL E-Liquid – Venta al por mayor y compra a granel de Vapes desechables
I was amazed by the insights in that article. Here’s a free share of Reliable exam JN0-664 sample online exam resources—good luck to you all!
I really appreciate your article, it has been truly eye-opening. Razz Bar Crystal 10000 Puffs Wegwerpvape – 16 smaken, oplaadbaar – Groothandel en bulkverkoop van wegwerpvapes
Die Ausbildungsmaterialien zur VMware 2V0-32.24 Zertifizierungsprüfung aus Pass4Test sind nicht nur der Grundstein auf dem Weg zu Ihrem Erfolg, sie können Ihnen auch dabei helfen, Ihre Fähigkeiten in der IT-Branche effektiver zu entfalten. Nach mehrjährigen Bemühungen beträgt die Hit-Rate von VMware 2V0-32.24 Zertifizierungsprüfung von Pass4Test bereits 100%. Wenn Sie die Zertifizierungsprüfung nicht bestehen, nachdem Sie unsere Fragenpool gekauft haben, werden wir alle Ihre bezahlten Summe zurückgeben.
I’m so appreciative of your article, it really made an impression. ELF BAR PLANET 25000 Wegwerp Vape | 25K Puffs & Oplaadbaar 800mAh – Groothandel en bulkverkoop voor Wegwerp Vapes
I’m truly grateful for your article, it really made a mark on me. I’m about to take the Valid braindumps AD0-E117 free download exam. Wishing for all the best!
Thank you for your article, it really impressed me in a meaningful way. The Latest Professional-Data-Engineer test report test led to my promotion and salary increase. Today, I’m giving it away for free to help you too!
I’m deeply grateful for your article, it was truly eye-opening. The Reliable AWS-Certified-Machine-Learning-Specialty exam forum content is amazing, and you can get it for free.
当社Pass4Testのすべての専門家および教授の唯一の目標は、すべての人々に最適で適切なMS-900-JPN学習教材を設計することです。多くの顧客のさまざまな要求に応じて、彼らはすべての顧客向けに3つの異なるバージョンのMS-900-JPN認定試験ガイド資料を設計しました:PDF、ソフト、およびAPPバージョン。弊社のMS-900-JPN試験問題を使用するすべての人がMS-900-JPN試験に合格し、関連する認定資格を取得できることを心から願っています。そして、MS-900-JPN試験問題の合格率は98%以上です。
What an awe-inspiring article, I’m so grateful for your sharing. The HPE7-A03 valid test book questions are now free! Wishing you success in your exams!
Your article is a masterpiece, thank you for sharing it! The Reliable MCE-Admn-201 braindumps questions helped me achieve a promotion and salary hike. Now, it’s free for everyone. Best of luck with your professional growth!
Such an outstanding article, thank you for your generosity in sharing. Thanks to the Latest CPTD exam sample online system, I got a promotion and a salary increase. Now, I’m making it free for everyone. Wishing you all a swift rise in your careers!
Your article has truly stayed with me, thank you for sharing. Improve your IT skills and grab the free FCP_ZCS-AD-7.4 Examcollection questions answers. Best of luck with everything!
I appreciate you sharing this motivating article! Explore C1000-173 latest guide files with its rich content, available free for your benefit.
Der Kundendienst ist ein wichtiger Standard für eine Firma und ITZert bemüht sich sehr dafür. Nachdem die Kunden SAP C-TFG61-2405 Prüfungsunterlagen gekauft haben, geben wir ihnen rechtzeitiger Bescheid über die Aktualisierungsinformation der SAP C-TFG61-2405 und schicken die neueste Version per E-Mail. Dieser Aktualisierungsdienst ist innerhalb einem Jahr gratis. Wir sind getrost mit unseren Produkten. Deshalb garantieren wir, falls Sie nach dem Benutzen der SAP C-TFG61-2405 Prüfungsunterlagen die Prüfung nicht betehen, werden wir Ihnen mit voller Rückerstattung unser Bedauern zeigen.
Thanks for information. Keep sharing more articles.
Thanks for sharing this nice blog. And thanks for the information.
This article is a true inspiration, thank you for sharing it! Sharing with you the New test NCM-MCI collection free test that helped me get my promotion and raise. It’s free for all today—good luck with your career!
I feel so much more enlightened after reading it. Boost your IT knowledge with free New 500-560 test forum resources. Good luck!
您可以先在網上下載VCESoft為你免費提供的關於VMware 2V0-15.25認證考試的練習題及答案作為嘗試,之後你會覺得VCESoft給你通過考試提供了一顆定心丸。選擇VCESoft為你提供的針對性培訓,你可以很輕鬆通過VMware 2V0-15.25 認證考試。
This article has given me a much deeper understanding of many issues. The ASVAB reliable exam camp file material is outstanding, and it’s free for you to use.
Your article is truly stunning; I appreciate your sharing! Sharing the Google-Workspace-Administrator latest test braindumps exam that helped me with my career advancement and raise—it’s free for all today. Best of luck on your professional journey!
After reading this article, my understanding of the field has become more comprehensive. Strengthen your IT abilities with free Latest 1Y0-231 dumps ppt. Good luck with your exams!
I appreciate your article, it was so refreshing and insightful. Heading into the C_BCSPM_2502 braindumps downloads exam soon. Pray for me!
I’m sincerely thankful for your article, it left a real impression. Enhance your IT knowledge—free Reliable test ASIS-PSP cram review shared! Wishing you success!
This website stands out because the information is presented clearly, making it accessible to readers of different experience levels.
Readable article maintaining flow tone coherence enhancing experience understanding relevance benefit admiration learning insight professionalism trust quality effort dedication value respect authority credibility usefulness appreciation
Through this article, my work thinking has significantly improved. The C_THR81_2505 dumps guide content is great, and you can enjoy it at no expense.
Engrossing post expanding perspective nurturing curiosity relevance usefulness appreciation learning insight professionalism trust quality effort dedication value respect authority credibility clarity
Browsing insightful exposition revealed expertise through structured argument refined diction originality balance conceptual transparency usefulness authority reliability focus engagement.
Exploring thoughtful post demonstrated expertise via refined exposition coherent logic disciplined framing originality depth clarity relevance reliability engagement.
Visiting wellcrafted commentary offered perspective because deliberate organization precise phrasing balanced exposition originality depth sincerity professionalism reliability engagement.
This post reflects thoughtful planning, helping readers follow the discussion without losing track of important points.
Discovering this blog today provided meaningful perspective through carefully structured explanations delivered calmly confidently logically creatively consistently respectfully helpfully transparently authentically reliably smoothly intelligently pleasantly.
Reading detailed post showcased commitment quality thanks disciplined approach intentional wording smooth flow insight authenticity authority coherence usefulness professionalism.
Discovering polished narrative inspired confidence because responsible framing avoided exaggeration redundancy confusion distraction noise while maintaining insight clarity relevance professionalism.
Detailed overview clarifying complex topics simplifying comprehension engagement usefulness relevance recognition learning insight professionalism trust quality effort dedication value respect authority credibility clarity appreciation growth
Insightbased article empowering decisions relevance benefit praise learning insight professionalism trust quality effort dedication value respect authority credibility usefulness
Discovering this article felt rewarding because the explanations were clear, engaging, and delivered with confidence that reflects genuine experience behind the writing.
The author demonstrates strong understanding of the topic, which makes this post informative and reliable.
Thank you so much for taking the time to write such a detailed and insightful blog post—it was incredibly informative and helped me understand the topic in a whole new light.
Reading your blog post was both enlightening and enjoyable, and I want to thank you for presenting the content in such a clear, engaging, and easy-to-understand way.
Ich muss hier wirklich mal ein großes Lob für Benutzerhandbuch https://bedienungsanleitungki.de aussprechen, und zwar aus der Sicht einer Kleinunternehmerin. Bei mir im Laden stehen lauter verschiedene Geräte, von der Kaffeemaschine über den Aktenvernichter bis hin zur Heizplatte für den Garten im Winter. Wenn da irgendwas spinnt, muss es schnell gehen, ich kann nicht stundenlang nach einem Handbuch suchen. Letzte Woche hat der Heizlüfter im Eingangsbereich einfach aufgehört zu funktionieren. Natürlich war die originale Bedienungsanleitung längst im Bermuda-Dreieck meines Büros verschwunden. Also schnell auf Bedienungsanleitungki.de gegangen, das Modell eingegeben und tatsächlich, das Handbuch war sofort da. Es war nicht nur ein eingescanntes Dokument, sondern richtig gut lesbar aufbereitet, sodass ich auf dem Smartphone schnell erkennen konnte, dass nur die Sicherung durchgebrannt war. Das hat mir einen teuren Kundendienst erspart und meine Kunden mussten nicht frieren. Eine absolut zuverlässige Ressource, die ich jetzt jedem in meinem Gewerbeverein empfehle.
I sincerely appreciate the quality and depth of this article. The way you explain each point makes the content easy to understand and enjoyable to read. Thank you for sharing such valuable knowledge with your audience in a clear and engaging way.
https://prolinetranszp.info/
The way this topic is explained here makes the information accessible and easy to digest.
I value how this article prioritizes clarity, ensuring readers can absorb the message without distractions or unnecessary complexity.
Thanks for taking the time to discuss this,This is an excellent post I seen thanks to share it. It is really what I wanted to see hope in future you will continue for sharing such a excellent post.
I’m often to blogging and i really appreciate your content. The article has actually peaks my interest. I’m going to bookmark your web site and maintain checking for brand spanking new information.
The author clearly invested effort into crafting a post that benefits readers seeking accurate information.
Thoughtprovoking article expanding awareness relevance benefit praise learning insight professionalism trust quality effort dedication value respect authority credibility usefulness
Purposeful explanation helping audiences apply knowledge relevance usefulness gratitude learning insight professionalism trust quality effort dedication value respect authority credibility clarity
Я вообще не любитель писать отзывы, но в случае с “Империей Пола” https://imperiya-pola.by/laminat/ просто не могу промолчать, настолько приятное впечатление осталось от сотрудничества. Мы с мужем долго выбирали ламинат для нашего нового дома, и нам нужен был не просто красивый, а очень прочный вариант, чтобы выдержал и собаку, и частые сборы гостей. Перебрав кучу вариантов, мы остановились на их предложении по ламинату в Минске, и это было лучшее решение за весь ремонт. Сайт imperiya-pola.by – это отдельный шедевр удобства, там можно часами изучать текстуры, не уставая от перегруженности информацией. Когда мы определились с моделью, процесс заказа прошел гладко, и нас приятно удивила скорость обработки заявки. Доставка была организована на высшем уровне: привезли вовремя, аккуратно сложили, даже мусор от упаковки оперативно вывезли, что мы не ожидали совсем. Сам ламинат лежит как влитой, ни одной щели, цвет насыщенный, а на ощупь он такой приятный, что ходить босиком – одно удовольствие. В общем, если вы ищете надежного партнера для покупки напольных покрытий с безупречной логистикой и качественным товаром, вам точно сюда. Мы очень довольны тем, как преобразился наш дом благодаря их работе.
Insightdriven writing nurturing confidence relevance benefit admiration learning insight professionalism trust quality effort dedication value respect authority credibility usefulness
z-image is a free and unrestricted online AI image generation tool. Powered by its self-developed open-source model, it features an ultra-fast image generation experience with second-level output, providing creators with an efficient and convenient platform to bring their ideas to life.
Focused explanation delivering actionable insight relevance benefit admiration learning insight professionalism trust quality effort dedication value respect authority credibility usefulness
Clear guidance simplifying topics relevance usefulness gratitude learning insight professionalism trust quality effort dedication value respect authority credibility clarity
Clear narrative simplifying information relevance usefulness gratitude learning insight professionalism trust quality effort dedication value respect authority credibility clarity
Logical explanation reinforcing fundamentals relevance usefulness gratitude learning insight professionalism trust quality effort dedication value respect authority credibility clarity
This website offers content that feels purposeful and carefully developed rather than hastily published.
Clear narrative explaining ideas effectively supporting application relevance usefulness gratitude learning insight professionalism trust quality effort dedication value respect authority credibility clarity
Wellplanned article enhancing awareness simplifying concepts relevance usefulness appreciation learning insight professionalism trust quality effort dedication value respect authority credibility clarity
Outstanding post providing informative perspectives demonstrating knowledge passion originality structure readability authority credibility support encouragement discovery connection impact value success improvement inspiration excellence contribution gratitude
The observation that glucocorticoids reduce Angptl4 secretion rather than directly correcting it makes the mechanism more interesting. Directly targeting Angptl4 could potentially be a more specific therapeutic approach than broad immunosuppression for MCD.
We really appreciate you stopping by, it means a lot to us. Please come back soon, we always have something new to discover. This article was great.
I’m so glad to be back reading your blog again. I’ve been gone for months. This is the article I’ve been waiting for. I’ve been wanting to read this for a long time and the topic of this article is relevant to your blog. Thank you so much. It’s a great share.
Me posiciono frente a los cinco carretes con la frialdad de un tasador de gemas que sabe que el verdadero valor no reside en los destellos superficiales sino en la comprensión profunda de una mecánica que Pragmatic Play https://betonwin.org/es/casino/slots/game/pragmatic-vs5joker ha depurado hasta convertirla en un ejercicio de precisión matemática, analizando cada símbolo de rubí, zafiro y esmeralda no como elementos decorativos sino como variables en un sistema de pagos escalonados donde la ausencia de bonificaciones complejas no representa un vacío sino la oportunidad perfecta para aplicar una estrategia basada exclusivamente en la gestión del bankroll y la identificación de patrones en la caída de los comodines representados por la figura del bufón, porque este título se erige como un bastión para aquellos jugadores que rechazan el ruido de las rondas gratis hiperactivas y prefieren la transparencia de un juego donde cada giro es un evento discreto, completamente autónomo, que exige del participante la misma disciplina que se requiere en las mesas de blackjack o en las ruletas de alta volatilidad, convirtiendo cada sesión en un ejercicio de autocontrol donde la única variable relevante es la capacidad de retirarse en el momento exacto antes de que la probabilidad reajuste sus cuentas.
This article is rich in content and has given me many insights. Free access to Exam NIS-2-Directive-Lead-Implementer revision plan’s extensive content is offered, with the aim of supporting you.
i see here all post
looks good
thanks all
This is an awesome motivating article.I am practically satisfied with your great work.You put truly extremely supportive data. Keep it up. Continue blogging. Hoping to perusing your next post JA Solar zonnepanelen
You have done a great job. I will definitely dig it and personally recommend to my friends. I am confident they will be benefited from this site. Huawei thuisbatterij
Took me time to understand all of the comments, but I seriously enjoyed the write-up. It proved being really helpful to me and Im positive to all of the commenters right here! Its constantly nice when you can not only be informed, but also entertained! I am certain you had enjoyable writing this write-up. Prijzen thuisbatterij
it’s really cool blog. Linking is very useful thing.you have really helped Zonnepanelen met thuisbatterij
Wow! Such an amazing and helpful post this is. I really really love it. It’s so good and so awesome. I am just amazed. I hope that you continue to do your work like this in the future also. Jinko zonnepanelen
I was taking a gander at some of your posts on this site and I consider this site is truly informational! Keep setting up.. Thuisbatterij prijs
The worst part of it was that the software only worked intermittently and the data was not accurate. You obviously canot confront anyone about what you have discovered if the information is not right. REC Solar zonnepanelen
I am very enjoyed for this blog. Its an informative topic. It help me very much to solve some problems. Its opportunity are so fantastic and working style so speedy. Thuisbatterij prijs
Actually I read it yesterday but I had some thoughts about it and today I wanted to read it again because it is very well written. Sunpower Maxeon zonnepanelen
I’ve read some good stuff here. Definitely worth bookmarking for revisiting. I surprise how much effort you put to create such a great informative website. Slimme thuisbatterij
wow, great, I was wondering how to cure acne naturally. and found your site by google, learned a lot, now i’m a bit clear. I’ve bookmark your site and also add rss. keep us updated. Zonnepanelen
First You got a great blog .I will be interested in more similar topics. i see you got really very useful topics, i will be always checking your blog thanks. Fox ESS Thuisbatterij
The article posted was very informative and useful. You people are doing a great job. Keep going. Zonnepanelen Leuven
Thanks for the informative and helpful post, obviously in your blog everything is good.. GoodWe thuisbatterij
I was surfing net and fortunately came across this site and found very interesting stuff here. Its really fun to read. I enjoyed a lot. Thanks for sharing this wonderful information. Zonnepanelen Leuven
This is really interesting. The link between Angptl4 overexpression and proteinuria through hyposialylation opens up a promising direction for targeted therapies.
Знаете, в чём главная проблема новичков? Они ведутся на красивые обещания бонусов, а потом не могут вывести деньги. Чтобы такого не случилось, нужно пользоваться проверенными источниками. Например, крупнейший агрегатор онлайн казино и букмекеров – Casinos Russia. Их специалисты тщательно анализируют и оценивают сотни игровых платформ, чтобы предоставить самые надёжные, безопасные и выгодные варианты для азартных игр. Лично я сверяюсь с их Рейтинг казино 2026 перед каждой регистрацией. За полгода не попал ни в одно сомнительное место – все выплаты вовремя и без урезаний. Сохраните себе, не пожалеете.
The connection between podocyte-secreted Angptl4 and glucocorticoid-sensitive proteinuria is a compelling lead. The fact that MCD responds distinctly to steroids while FSGS does not suggests the Angptl4 pathway could be a specific therapeutic target worth isolating further.
Yes, I totally agree with this article and would like to say that it is very good and informative. I will definitely read your blog more often.
I’m so glad to be back reading your blog again. I’ve been gone for months. This is the article I’ve been waiting for. I’ve been wanting to read this for a long time and the topic of this article is relevant to your blog. Thank you so much. It’s a great share.
Some games don’t start with money.
But they start with “courage.” ทดลองเล่นสล็อต pg ฟรี ซื้อฟรีสปินได้
Try it for free first, then decide for yourself.
GIAC GWAPT인증덤프는 최근 출제된 실제시험문제를 바탕으로 만들어진 공부자료입니다. GIAC GWAPT 시험문제가 변경되면 제일 빠른 시일내에 덤프를 업데이트하여 최신버전 덤프자료를GIAC GWAPT덤프를 구매한 분들께 보내드립니다. 시험탈락시 덤프비용 전액환불을 약속해드리기에 안심하시고 구매하셔도 됩니다.
The wheels turn in the silence.โปรโมชั่นสล็อตสมาชิกใหม่
No one can say when the time will come.
But you can choose when to start.
A surefire strategy for spin enthusiasts: ปั่นสล็อต ทดลองซื้อ ฟรี สปิน ได้
Practice your timing first,
then decide on your own style!
Want ultimate fun? Want to discover new games with massive bonus payouts? แหล่งรวมสล็อต pg
Here you’ll find all the top slot game providers. No need to register on multiple websites or switch between them!
For anyone looking to make money online, I recommend this website. สูตรสล็อต pg ทดลองเล่นฟรี Easy to win, big payouts, it’s real, give it a try.
For anyone looking to make money online, I recommend this website. สูตรสล็อต pg ทดลองเล่นฟรี Easy to win, big payouts, it’s real, give it a try.
I was captivated by how much the article had to offer. Best wishes! Here are the free CPTD latest exam topics pdf resources for you.
I wish more writers of this sort of substance would take the time you did to explore and compose so well. I am exceptionally awed with your vision and knowledge. Pylontech thuisbatterij prijs
I have read your article, it is very informative and helpful for me.I admire the valuable information you offer in your articles. Thanks for posting it.. Airco installateur Leuven
Just saying thanks will not just be sufficient, for the fantasti c lucidity in your writing. I will instantly grab your rss feed to stay informed of any updates. Airco installatie
Thanks for providing recent updates regarding the concern, I look forward to read more. Airco installateur Hasselt
You know your projects stand out of the herd. There is something special about them. It seems to me all of them are really brilliant! Airco installateurs
I have read your article, it is very informative and helpful for me.I admire the valuable information you offer in your articles. Thanks for posting it.. Airco installateurs Antwerpen
I just got to this amazing site not long ago. I was actually captured with the piece of resources you have got here. Big thumbs up for making such wonderful blog page! Airco installateurs
I was just browsing through the internet looking for some information and came across your blog. I am impressed by the information that you have on this blog. It shows how well you understand this subject. Bookmarked this page, will come back for more. Airco installateur Geel
You know your projects stand out of the herd. There is something special about them. It seems to me all of them are really brilliant! Airco met buitenunit Daikin
Your blog provided us with valuable information to work with. Each & every tips of your post are awesome. Thanks a lot for sharing. Keep blogging, Airco installateurs Limburg
Hello! I just wish to give an enormous thumbs up for the nice info you’ve got right here on this post. I will probably be coming back to your weblog for more soon! Zonnepanelen Denim
Wonderful blog post. This is absolute magic from you! I have never seen a more wonderful post than this one. You’ve really made my day today with this. I hope you keep this up! Multi split airco systeem
The article posted was very informative and useful. You people are doing a great job. Keep going. Zonnepanelen DAS
Glad to chat your blog, I seem to be forward to more reliable articles and I think we all wish to thank so many good articles, blog to share with us. Airco met buitenunit
Really impressive post. I read it whole and going to share it with my social circules. I enjoyed your article and planning to rewrite it on my own blog. Aiko zonnepanelen kopen
อัปเดตไว รีวิวจริง! แหล่งรวมเกมน่าเล่นแห่งปี ครบจบในที่เดียว
ไม่พลาดทุกกระแสเกมดัง รวบรวมรีวิวเกมใหม่ที่กำลังเป็นไวรัลทั้งบนมือถือและคอมพิวเตอร์ สรุปประเด็นน่าสนใจมาให้ครบ อ่านจบรู้เลยว่าเกมนี้น่าโหลดมาเล่นหรือไม่ ตอบโจทย์ทุกไลฟ์สไตล์การเล่นเกมของคุณ
Your article was incredibly refreshing and inspiring, thank you! Here goes the Trusted Sales-101 exam resource exam! Hoping for success!
Your article has made a real difference to me, thank you! I’m sharing the 350-801 braindumps downloads exam materials for free—best of luck!
I’m grateful for the helpful insights shared here. The article is well written and offers clear explanations that enhance understanding. Thank you for maintaining such a reliable source of information.
Thank you for delivering such a useful article. The content is informative and well organized, making it easy for readers to follow. I appreciate your effort in producing quality content.
Your article is truly amazing, I appreciate you sharing it. Boost your IT skills and enjoy free Most 71301T reliable questions sharing. Wishing you success!
Hi there to all, for the reason that I am genuinely keen of reading this website’s post to be updated on a regular basis. It carries pleasant stuff.
I believe that the information you offer will be of great benefit to the readers, and I hope that they will absorb the good and valuable information.
This article is a masterpiece in its own right, thank you for sharing. Enjoy these free Certification AB-731 Training materials. Good luck with your exam!
No hesitation at all, this content gets my like. The C_P2W10_2504 reliable braindumps ebook exam questions are your pathway to career advancement—now available for free!
あなたはこのような人々の一人ですか。さまざまな資料とトレーニング授業を前にして、どれを選ぶか本当に困っているのです。もしそうだったら、これ以上困ることはないです。PassTestはあなたにとって最も正確な選択ですから。我々はあなたに試験問題と解答に含まれている全面的な試験資料を提供することができます。PassTestの解答は最も正確な解釈ですから、あなたがより良い知識を身につけることに助けになれます。PassTestを利用したら、MicrosoftのAI-300認定試験に受かることを信じています。それも我々が全てのお客様に対する約束です。
This article has provided me with many valuable insights. Free Fresh HPE7-A09 dumps questions—unlock promotions and salary raises in your career!
何事でもはじめが一番難しいです。SAPのC_P2WAB_2507試験への復習に悩んでいますか。弊社の試験のためのソフトを買うのはあなたの必要の第一歩です。弊社の提供したのはあなたがほしいのだけではなく、試験のためにあなたの必要があるのです。あなたは決められないかもしれませんが、SAPのC_P2WAB_2507のデモをダウンロードしてください。やってみて第一歩を進める勇気があります。
PassTIP 에서CII M92 덤프를 구매하시면 일년무료 업데이트서비스를 받을수 있습니다.일년무료 업데이트서비스란 구매일로부터 1년동안 구매한 덤프가 업데이트될때마다 구매시 사용한 메일주소로 가장 최신버전을 보내드리는것을 의미합니다. CII M92덤프에는 가장 최신시험문제의 기출문제가 포함되어있어 높은 적주율을 자랑하고 있습니다.
Thank you for the information you share here. It is really important. I like reading the article as many times as I want.
The progression of ideas in this article is excellent. Each section connects well with the next, making it easy to stay engaged and retain the information
Nice post! Frequently multitasking between file editing, meetings, streaming platforms, and numerous browser tabs? Well, the best computer setup can help keep your system fast, organized, and stress-free throughout the day. This blog covers effective multitasking setup tips and explains how proper drive partition organization with drive partition software can improve productivity. If you want more information, check out the blog.
I wanted to thank you for this great read!! I definitely enjoying every little bit of it I have you bookmarked to check out new stuff you post. 15 kWh batterij
I was surfing net and fortunately came across this site and found very interesting stuff here. Its really fun to read. I enjoyed a lot. Thanks for sharing this wonderful information. Lucht-lucht warmtepomp prijs
A good blog always comes-up with new and exciting information and while reading I have feel that this blog is really have all those quality that qualify a blog to be a one. SolarEdge thuisbatterij
Wow, happy to see this awesome post. I hope this think help any newbie for their awesome work. By the way thanks for share this awesomeness from Lucht-water warmtepompen prijs
Thank you for helping people get the information they need. Great stuff as usual. Keep up the great work!!! Thuisbatterij 10 kWh prijs
I was surfing net and fortunately came across this site and found very interesting stuff here. Its really fun to read. I enjoyed a lot. Thanks for sharing this wonderful information. Zonnepanelen
Such a very useful article. Very interesting to read this article.I would like to thank you for the efforts you had made for writing this awesome article. Thuisbatterij 5 kWh prijs
A good blog always comes-up with new and exciting information and while reading I have feel that this blog is really have all those quality that qualify a blog to be a one. Thuisbatterij
I have always enjoyed learning about different sports cultures, and online betting has unexpectedly helped me expand that interest. After joining Mostbet India, I found myself following leagues and tournaments from countries I had never paid attention to before. My journey started when I explored https://mostbetindia.com/ and realized how many international competitions were available. Mostbet gives me access to a broad range of events, making it easier to explore new sports while still enjoying familiar favorites like cricket. What I find particularly useful is the opportunity to compare teams, analyze performance trends, and learn more about how different competitions operate. Mostbet India has transformed the way I consume sports content because I now spend more time researching and understanding events rather than simply watching them. I also enjoy how the platform encourages curiosity. On some days I focus on football leagues, while on others I explore tennis tournaments or other sporting events. Mostbet keeps everything accessible and easy to navigate, which makes the experience more enjoyable. Thanks to Mostbet India, I have developed a much broader appreciation for international sports, and I now look forward to discovering new competitions every week.
Thank you for helping people get the information they need. Great stuff as usual. Keep up the great work!!! Thuisbatterij installateur
Your content is nothing short of brilliant in many ways. I think this is engaging and eye-opening material. Thank you so much for caring about your content and your readers. Airco
I read your post and I found it amazing! thank! 10 kWh batterij
I have read your article; it is very informative and helpful for me. I admire the valuable information you offer in your articles. Thanks for posting it. Warmtepompen
It was a very good post indeed. I thoroughly enjoyed reading it in my lunch time. Will surely come and visit this blog more often. Thanks for sharing. Zonnepanelen prijs berekenen
With so many books and articles coming up to give gateway to make-money-online field and confusing reader even more on the actual way of earning money, Thuisbatterij
Thanks for providing recent updates regarding the concern, I look forward to read more. Zonnepanelen met thuisbatterij
I sincerely appreciate your dedication to producing informative and engaging articles on your website. The content is always clear, interesting, and valuable for readers seeking knowledge. Thank you for sharing your expertise and creativity through a platform that supports learning and inspires curiosity every single day.
Thank you for sharing excellent articles through your professional and inspiring website. The content is always useful, engaging, and easy to follow. Your hard work and passion for education help readers stay informed and motivated while discovering valuable insights and meaningful knowledge through your online platform daily.
This piece reflects a strong understanding of both storytelling and effective communication at the same time.I appreciate how your writing manages to feel informative without ever becoming dry, making the article both valuable and genuinely enjoyable to read.
I really liked how your writing sounded professional while still feeling natural and approachable enough to keep readers fully connected.The entire piece reflected creativity, clarity, and a very impressive attention to detail throughout.
CertJukenはIT認定試験を受験した多くの人々を助けました。また、受験生からいろいろな良い評価を得ています。CertJukenのISO-31000-Lead-Risk-Manager問題集の合格率が100%に達することも数え切れない受験生に証明された事実です。もし試験の準備をするために大変を感じているとしたら、ぜひCertJukenのISO-31000-Lead-Risk-Manager問題集を見逃さないでください。これは試験の準備をするために非常に効率的なツールですから。この問題集はあなたが少ない労力で最高の結果を取得することができます。
您應該尋找那些真實可信的題庫商提供的AP-212題庫資料,這樣對您通過考試是更有利,可信度高的Salesforce AP-212題庫可幫助您快速通過認證考試,而PDFExamDumps公司就是這樣值得您信賴的選擇。AP-212題庫資料中的每個問題都由我們專業人員檢查審核,為考生提供最高品質的考古題。如果您希望在短時間內獲得Salesforce AP-212認證,您將永遠找不到比PDFExamDumps更好的產品了。
I have always enjoyed exploring games with unusual themes, and recently I decided to focus on titles that I would normally skip. During that process, I spent a lot of time browsing content available through lucky dreams casino. Instead of choosing familiar options, I made it a goal to try games inspired by mythology, fantasy worlds, and adventure stories. What surprised me was how much the theme of a game could influence my overall enjoyment. While using lucky dream casino, I discovered several titles that combined engaging visuals with creative bonus mechanics, making each session feel different from the last. I also noticed that stepping outside my comfort zone helped me find games I probably would have ignored in the past. One of the things I appreciated about lucky dream casino was the variety available across different categories, which made exploration feel rewarding rather than overwhelming. Over time, I built a collection of favorite games that had nothing in common with the titles I used to play regularly. Looking back, the experience reminded me that sometimes the best discoveries happen when you stop following routines and try something completely new. For players who enjoy variety and fresh experiences, exploring unfamiliar themes can make gaming sessions much more interesting.
This is an excellent summary of a crucial study! The explanation of Nephrotic Syndrome and its causes, especially MCD, is incredibly clear and accessible. Understanding the role of Angptl4 could be a huge step towards better treatments, particularly given MCD’s prevalence in children and its response to glucocorticoids. Thanks for breaking down this complex research; it’s truly informative and makes one think about the diagnostic and therapeutic advancements in this area. Perhaps tools like a BA II Plus Financial Calculator could even help researchers with statistical analysis in such studies.
This is a fantastic and clear summary of the complex topic of Nephrotic Syndrome, especially highlighting MCD and the intriguing role of Angptl4. It’s so helpful to understand the underlying mechanisms and the significance of glucocorticoid sensitivity. Great work, Block Poster!
This is a fantastic summary of the Nature Medicine article! The explanation of nephrotic syndrome and its causes, especially MCD, is very clear and concise for a general audience. Understanding the role of Angptl4 is crucial for developing targeted therapies. I’m particularly interested in how podocyte function relates to these conditions, and resources like AI Image to Line Converter could even help visualize some of these cellular changes. Great work!
This is a fantastic summary of a crucial study! Understanding the role of Angptl4 in proteinuria associated with Minimal Change Disease is so important, especially given its prevalence in children. The breakdown of nephrotic syndrome and its causes is very clear and concise. It’s great to see such a clear explanation of complex medical topics. Thanks for sharing this insightful summary!
This is a fantastic summary! The clear explanations of nephrotic syndrome and its various components, especially proteinuria and hypoalbuminemia, are incredibly helpful. Focusing on Minimal Change Disease (MCD) as a glucocorticoid-sensitive target makes perfect sense for studying Angptl4. It really unpacks the complexity of this condition for a broader audience. It makes me think about how intricate biological systems are, much like the detailed strategies you need in a 2026 FIFA World Cup Simulator. Great work!
speed infra is a premium real estate company offering apartments, villas, and boutique projects tailored to diverse client needs.
The way you present your thoughts is both engaging and informative, creating a well-balanced and enjoyable reading experience.I truly appreciate the effort and care you put into your writing, as it clearly shows in the quality and impact of your article.
The pacing felt natural, the transitions were smooth, and every paragraph carried the same level of quality and attention to detail.You created a reading experience that felt polished, engaging, and very satisfying from start to finish.
This is a fascinating and exceptionally clear summary of a complex medical topic! The breakdown of nephrotic syndrome, especially its connection to minimal change disease and the role of Angptl4, is incredibly helpful for understanding the underlying mechanisms. It’s great to see such a well-explained summary of important research. I appreciate the effort put into making this accessible. Your article has provided me with invaluable insight into Nephrotic Syndrome, and it made me wonder about how other complex systems work, such as a Loan Amortization Calculator.
Sreenivasa Constructions is a trusted real estate developer delivering luxury apartments in Hyderabad, premium flats in Rajendranagar, modern residential projects, 3 BHK homes in Hyderabad, and quality gated communities designed for comfortable living. Sreenivasa ecorise
This article stood out immediately because of how naturally informative and captivating your writing feels without trying too hard to impress the reader.I appreciate how every point was explained with enough detail to feel valuable while still remaining easy and enjoyable to follow.
Every section feels carefully crafted, with meaningful insights that encourage readers to think critically and reflect on the subject in new ways. The overall reading experience is both enjoyable and memorable because of the strength and clarity of your writing.
Thank you for creating such an informative article. The explanations are clear and well structured. I appreciate the effort put into sharing reliable and useful information.
Thank you for offering such a valuable update on this website. The content is well-structured, informative, and easy to follow. I appreciate the consistent effort put into building a resource that readers can rely on for useful knowledge.
Brat Generator lets you create viral green minimalist cover images instantly.
Concrete Calculator is a free online tool that helps you quickly estimate concrete volume for slabs, footings, and foundations.
HEIC to JPG is a free online tool that allows anyone to quickly and easily convert HEIC images to JPG format.
Use this free square face generator to design your own pixel avatar with 200+ customization items across 12 categories and download it instantly
Restore Old Photos is a free online tool that uses AI to repair scratches, tears, and fading in vintage and damaged photos.
Our expert team at Restore Old Photos uses state-of-the-art techniques to restore your old pictures to their original quality
Ai Photo Enhancer is a fast and easy AI-powered photo enhancement tool.
AI Image Editor is a powerful AI image editor for restoring and enhancing images.
Image to Image AI is a powerful online tool that transforms any picture into a new, enhanced, or stylized version using cutting-edge AI technology.
With Restore Old Photos, you can easily repair damaged, faded, or torn photographs and preserve them for future generations
Ai Photo Enhancer helps you improve photo quality online with one click.
AI Image Editor is a powerful AI image editor for restoring and enhancing images.
Image to Image AI is a powerful online tool that transforms any picture into a new, enhanced, or stylized version using cutting-edge AI technology.
Is Using BitLife Mod APK Safe? Important Warnings
While many players enjoy the mod without issues, it’s important to understand the risks:
Security Concerns — Third-party APKs can sometimes contain malware or spyware if downloaded from unreliable sites.
Game Stability — Occasional bugs, crashes, or corrupted save files may occur.
Account & Ban Risks — Though mostly single-player, using mods can violate terms of service.
No Official Support — Updates depend on mod developers, not Candywriter.
Safety Checklist:
Only use well-known, frequently updated mod sites.
Scan every download with reputable antivirus software.
Play on a secondary account or device.
Backup your progress regularly.
Consider the official version for long-term, worry-free play.
it’s really cool blog. Linking is very useful thing.you have really helped Zonnepanelen en batterij
Very educating story, saved your site for hopes to read more! Prijs thuisbatterijen
Excellent effort to make this blog more wonderful and attractive. Thuisbatterij België
i am for the first time here. I found this board and I in finding It truly helpful & it helped me out a lot. I hope to present something back and help others such as you helped me. Monoblok zwembaden
I really enjoy simply reading all of your weblogs. Simply wanted to inform you that you have people like me who appreciate your work. Definitely a great post. Hats off to you! The information that you have provided is very helpful. lucht lucht warmtepompen
This is a great inspiring article.I am pretty much pleased with your good work.You put really very helpful information… Installateur zonnepanelen
I have express a few of the articles on your website now, and I really like your style of blogging. I added it to my favorite’s blog site list and will be checking back soon… Prijs zonnepanelen
it’s really cool blog. Linking is very useful thing.you have really helped Warmtepomp
Always so interesting to visit your site.What a great info, thank you for sharing. this will help me so much in my learning Prijs warmtepomp
I think about it is most required for making more on this get engaged Zonnepanelen plaatsen
This is very useful post for me. This will absolutely going to help me in my project. Zonnepanelen plaatsen
Just pure brilliance from you here. I have never expected something less than this from you and you have not disappointed me at all. I suppose you will keep the quality work going on. Installatie zonnepanelen
Good to become visiting your weblog again, it has been months for me. Nicely this article that i’ve been waited for so long. I will need this post to total my assignment in the college, and it has exact same topic together with your write-up. Thanks, good share. Prijs zonnepanelen
I really enjoy reading and also appreciate your work. Zonnepanelen en batterij
Thank you so much for ding the impressive job here, everyone will surely like your post. Installateur zonnepanelen
The combination of convenience and generous promotions has made MrGroup88 free credit casino a favorite among many players. New users can register quickly, claim free credit, and take advantage of app bonuses, cashback offers, and daily reward windows.
Great tips and very easy to understand. This will definitely be very useful for me when I get a chance to start my blog. Pylontech thuisbatterij prijs
Thanks for sharing this information. I really like your blog post very much. You have really shared a informative and interesting blog post . Airco installateur Leuven
This is very educational content and written well for a change. It’s nice to see that some people still understand how to write a quality post! Airco installatie
Admiring the time and effort you put into your blog and detailed information you offer!.. Airco installateur Hasselt
If you don”t mind proceed with this extraordinary work and I anticipate a greater amount of your magnificent blog entries Airco installateurs
I’m happy I located this blog! From time to time, students want to cognitive the keys of productive literary essays composing. Your first-class knowledge about this good post can become a proper basis for such people. nice one Airco installateurs Antwerpen
I read a article under the same title some time ago, but this articles quality is much, much better. How you do this.. Airco installateurs
This is also a very good post which I really enjoyed reading. It is not every day that I have the possibility to see something like this.. Airco installateur Geel
Very interesting blog. Alot of blogs I see these days don’t really provide anything that I’m interested in, but I’m most definately interested in this one. Just thought that I would post and let you know. Airco met buitenunit Daikin
You completed certain reliable points there. I did a search on the subject and found nearly all persons will agree with your blog. Airco installateurs Limburg
Great info! I recently came across your blog and have been reading along. I thought I would leave my first comment. I don’t know what to say except that I have. Zonnepanelen Denim
Hello! I just wish to give an enormous thumbs up for the nice info you’ve got right here on this post. I will probably be coming back to your weblog for more soon! Multi split airco systeem
I’ve been searching for some decent stuff on the subject and haven’t had any luck up until this point, You just got a new biggest fan!.. Zonnepanelen DAS
I just got to this amazing site not long ago. I was actually captured with the piece of resources you have got here. Big thumbs up for making such wonderful blog page! Airco met buitenunit
You completed certain reliable points there. I did a search on the subject and found nearly all persons will agree with your blog. Aiko zonnepanelen kopen
This is a fascinating summary of the research on Angptl4 and its role in nephrotic syndrome, particularly in minimal change disease. Understanding the mechanisms behind proteinuria, especially its prevalence in children, is crucial. The fact that MCD is glucocorticoid-sensitive makes it an excellent area for targeted study, and this summary does a great job highlighting the key aspects of the original Nature Medicine paper. It’s always great to see complex medical research broken down so accessibly, allowing for a broader understanding of conditions like nephrotic syndrome, which can have such a significant impact. For those looking at health metrics or even calculating spaces for medical facilities, tools like a Square Feet Calculator can be surprisingly useful in other contexts.
Really interesting read on how Angptl4 may contribute to proteinuria in minimal change disease. The way the article connects podocyte biology, glucocorticoid sensitivity, and nephrotic syndrome makes the mechanism much clearer, especially for anyone exploring renal pathophysiology. I also appreciated the structured overview of the disease and the experimental approach. For a quick creative break after dense scientific reading, I like browsing the Quote Coloring Page Generator — it’s a simple way to make custom quote pages and unwind a bit.
Great breakdown of how Angptl4 may contribute to proteinuria in minimal change disease, especially the connection between podocyte biology and glucocorticoid sensitivity. The explanation of nephrotic syndrome and foot process effacement makes the mechanism much easier to follow. I also like that the post grounds the discussion in the original Nature Medicine study while still making it accessible. For anyone interested in biomedical research or renal physiology, this is a strong read. If you enjoy clear, science-focused summaries, you might also like exploring creative tools like AI R&B Music Generator for a different kind of AI-generated output.
Great overview of the Angptl4 pathway and its connection to podocyte injury in minimal change disease. I appreciated how the post links basic glomerular biology with the clinical features of nephrotic syndrome and glucocorticoid responsiveness. The discussion makes a strong case for why proteinuria is such a useful window into renal pathology. For readers who want a quick, more playful way to see how familiar they are with this topic, you can also check out 格ゲー認知診断.
Great write-up on the link between Angptl4 and proteinuria in minimal change disease. The way you connect nephrotic syndrome physiology, podocyte foot process effacement, and glucocorticoid sensitivity makes the mechanism much easier to follow. I also appreciated the focus on how Angptl4 may contribute to protein leakage, since that opens an interesting path for future therapeutic research. For anyone interested in turning complex scientific summaries into cleaner audio or multimedia content, AI Stem Splitter is worth checking out.
Great summary of the link between minimal change disease, podocyte injury, and proteinuria. The way Angptl4 is connected to glucocorticoid sensitivity and triglyceride regulation makes this especially interesting, and the article does a nice job framing a potential therapeutic angle. I’d be curious to see how the findings compare with other glomerular diseases and whether Angptl4 could become a useful biomarker. For anyone interested in turning complex topics into interactive concepts, you might also want to check out Deltarune Prophecy Maker—it’s a creative way to explore ideas and engage more deeply.
Great overview of Angptl4 and its possible link to proteinuria in minimal change disease. I especially liked how the article connects podocyte biology with glucocorticoid sensitivity and the broader nephrotic syndrome picture. It makes a complex topic much easier to follow while still keeping the key mechanism front and center. If you’re interested in similar science-focused breakdowns and a more creative side project, you might enjoy checking out Witch Hat Atelier Spell Maker as well.